Transparency and Record Keeping
HMIA 2025

"Lead is an essential element in car batteries. But mining and processing it is expensive. So companies have turned to recycling as a cheaper, seemingly sustainable source of this hazardous metal.
As the United States tightened regulations on lead processing to protect Americans over the past three decades, finding domestic lead became a challenge. So the auto industry looked overseas to supplement its supply. In doing so, car and battery manufacturers pushed the health consequences of lead recycling onto countries where enforcement is lax, testing is rare and workers are desperate for jobs.
...
The auto industry touts battery recycling as an environmental success story. Lead from old batteries, when recycled cleanly and safely, can be melted down and reused again and again with minimal pollution.
But companies have rejected proposals to use only lead that is certified as safely produced. Automakers have excluded lead from their environmental policies.
Battery makers rely on the assurances of trading companies that lead is recycled cleanly. These intermediaries rely on perfunctory audits that make recommendations, not demands.
The industry, in effect, built a global supply system in which everyone involved can say someone else is responsible for oversight.
Describe a time when things in your life (or recollection) went badly because there were no written records or when you were saved (or a story you can remember about someone else) by the fact that there was a written record.
Utah and California have passed laws requiring entities to disclose when they use AI. More states are considering similar legislation. Proponents say labels make it easier for people who don't like AI to opt out of using it.
"They just want to be able to know," says Utah Department of Commerce executive director Margaret Woolley Busse, who is implementing new state laws requiring state-regulated businesses to disclose when they use AI with their customers.
"If that person wants to know if it's human or not, they can ask. And the chatbot has to say."
California passed a similar law regarding chatbots back in 2019. This year it expanded disclosure rules, requiring police departments to specify when they use AI products to help write incident reports.
Transparency and Record Keeping
One of the central obstacles to alignment among intelligent agents—human or artificial—is the inscrutability of inner states and the opacity of the world: we cannot know what others are thinking, nor can we see everything that happens. Because intentions, reasoning, and perceptions are hidden—and even our own memories are fallible—alignment depends on creating external traces of cognition and action that others can inspect, verify, and learn from.
Transparency and recordkeeping counter the misalignment potential of secrecy, obscurity, and opacity. They make behavior visible, accountable, and interpretable across time and context. Records, disclosures, reporting requirements, and audits allow agents to see what is happening and what has happened; checklists proactively ensure that what will happen remains visible and verifiable. Together, these mechanisms transform private judgment into shared evidence, supporting trust, coordination, and corrigibility within complex systems.
.
Records
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
Disclosures
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
Disclosures
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
Reporting requirements
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
Audits
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
Checklists
A xxx is a mechanism that
LOREM
Human Interaction
lorem ipsum
Organizational
Lorem ipsum
Legal/Political
lorem ipsum
Professional/Expert
Lorem ipsum
Machines
Lorem Ipsum
THE READINGS
The piece explains how modern intensive care has pushed the boundaries of human survival—keeping patients alive through ventilators, dialysis, ECMO, feeding lines, and more—while creating a new problem: extreme complexity that routinely overwhelms even elite clinicians. Two vivid cases frame the point. A three-year-old Austrian girl is pulled pulseless from an icy pond after roughly two hours without a heartbeat; a tightly choreographed sequence—bypass, ECMO, sterile lines, pressure control, ventilation, neuro-monitoring—brings her all the way back. By contrast, a 48-year-old man with liver injury survives multi-organ failure but nearly dies from infections introduced via his life-sustaining lines—an emblem of how easily complex care harms as it heals.
Scale and fragility define the ICU. On any given day in the U.S., ~90,000 people are in intensive care; across a lifetime, most of us will see it from the inside. The average ICU stay is four days and survival is ~86%, but each patient requires ~178 distinct actions per day and teams still make about a 1% error rate—roughly two errors daily per patient. The risks compound over time: after 10 days, ~4% of central lines become infected (80,000 cases/year, with 5–28% mortality), ~4% of urinary catheters cause bladder infection, and ~6% of ventilated patients develop pneumonias with 40–55% mortality. ICU medicine works only when the odds of harm are kept consistently below the odds of benefit—no small feat amid alarms, crises next door, and fatigue.
Medicine’s reflexive answer to complexity has been ever deeper specialization—“intensivists” for the ICU, fellowships on fellowships. But the article argues that expertise alone cannot tame this level of complexity. Drawing an analogy from aviation’s “B-17 moment,” it recounts how Boeing’s revolutionary bomber first crashed due to “pilot error” born of complexity. The fix was not more heroics but a humble tool: the pilot’s checklist. With stepwise checks for takeoff, flight, landing, and taxiing, crews subsequently flew 1.8 million miles accident-free; the B-17 became a World War II workhorse.
Peter Pronovost’s work at Johns Hopkins brings that aviation lesson to the ICU. He started with one narrow, deadly problem: central-line infections. His five-step insertion checklist—wash hands; chlorhexidine skin prep; full sterile drape; sterile mask/hat/gown/gloves; sterile dressing—codified well-known basics. Yet when nurses observed physicians, at least one step was skipped in over a third of insertions. Empowering nurses to halt non-compliant procedures and to prompt daily line removal reviews drove the line-infection rate from 11% to ~0% at Hopkins, preventing dozens of infections and deaths and saving millions.
Could that work “in the wild”? In Michigan’s Keystone Initiative, hospitals paired checklists with executive support to fix supply gaps (chlorhexidine soap, full drapes) and vendor kits, tracked infection data, and sustained practice. Within three months, ICU line infections fell 66%; many units hit zero and stayed there. Over 18 months, the program saved an estimated 1,500 lives and $175 million. Parallel ventilator and pain-management checklists cut pneumonias, untreated pain, and ICU length of stay.
Why the resistance? Checklists can feel like an affront to professional audacity—the “right stuff” culture that valorizes improvisation under fire. But the article emphasizes that checklists don’t replace judgment; they reserve scarce cognitive bandwidth for the parts that truly require it, standardizing the mundane yet critical steps most vulnerable to omission. The larger indictment is that the “science of delivery”—how to ensure therapies are reliably executed—has been neglected relative to discovery and treatment science. For a few million dollars and national coordination, Pronovost estimates, line-infection checklists could be rolled out across U.S. ICUs; Spain, he notes, is moving faster.
The takeaway: in domains where lives hinge on intricate sequences, checklists are a deceptively powerful technology. They convert individual expertise into team reliability, reduce avoidable harm, and create the conditions in which skill and courage actually matter most. The question is less whether they work than whether medicine will accept the cultural shift from heroic memory to disciplined execution.
Which statement best captures the article’s central takeaway?
A. ICU outcomes improve primarily by adding more sub-specialists with longer training.
B. Checklists standardize critical but easily overlooked steps, enabling teams to manage ICU complexity more safely without replacing clinical judgment.
C. Most ICU harm comes from rare, unforeseeable equipment failures, so technology upgrades are the main solution.
D. Checklists are useful only in aviation because patients are too variable for medicine to benefit.
AI SUMMARY
A. To provide detailed technical specifications for model
replication and performance optimization.
B. To document and communicate a model’s intended uses,
performance across relevant groups, and ethical
considerations.
C. To ensure that models comply with open-source licensing
requirements.
D. To certify that a machine learning model has been
approved for deployment in sensitive domains.
According to Mitchell et al. (2019), “Model Cards for Model Reporting,” what is the primary purpose of a model card?
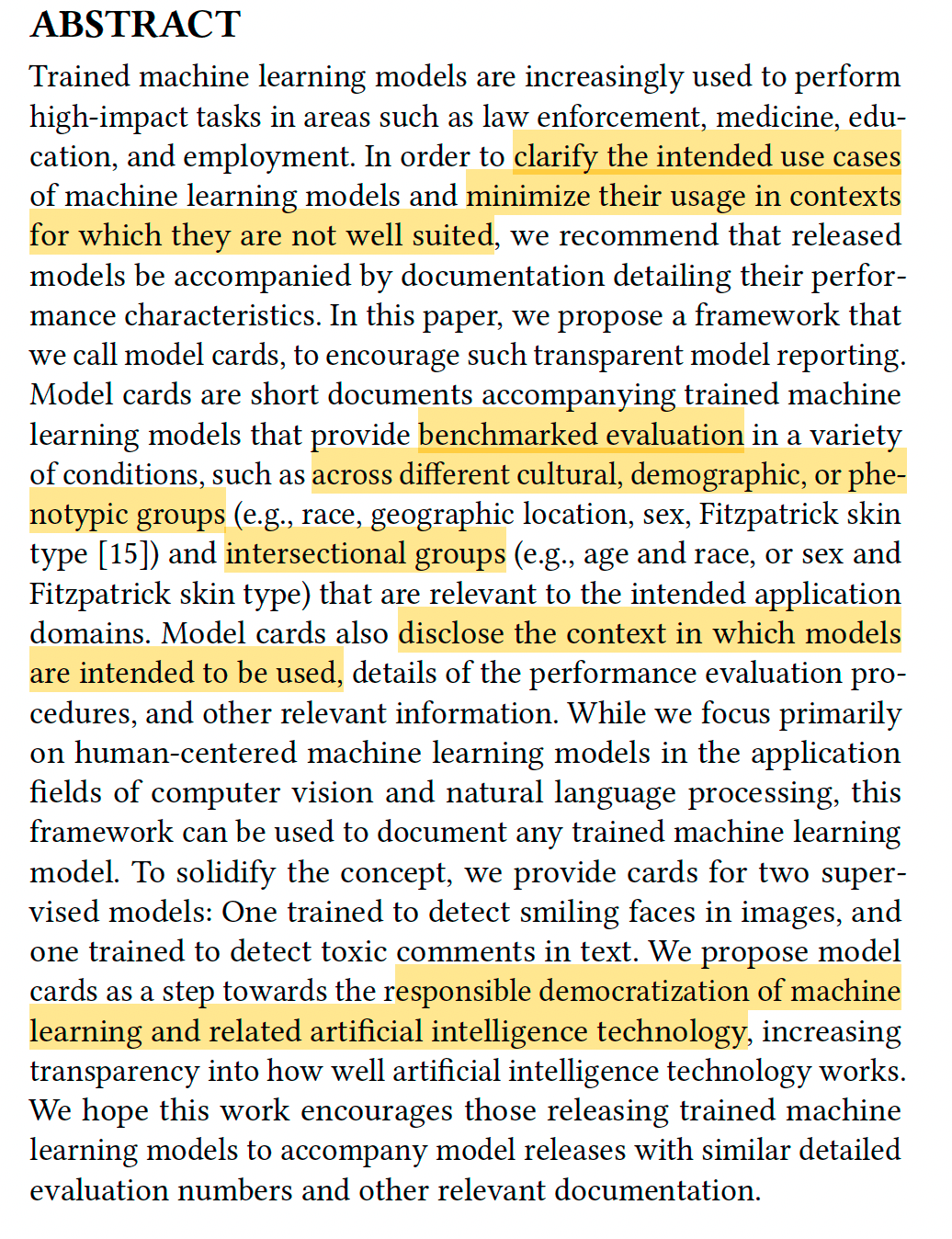
In “Model Cards for Model Reporting” (2019), Margaret Mitchell and colleagues propose a standardized framework for documenting machine learning models to improve transparency and accountability. Model cards are short documents that accompany trained models, summarizing their intended uses, limitations, and performance across different demographic, cultural, or phenotypic groups. By making these details explicit, model cards help developers, policymakers, and users understand how models work, where they might fail, and how biases or fairness issues could affect outcomes. The authors present model cards as an essential tool for promoting responsible AI development and for aligning technical practice with ethical and social values.
According to Mitchell et al. (2019), “Model Cards for Model Reporting,” what is the primary purpose of a model card?
CONCEPTS AND TERMS
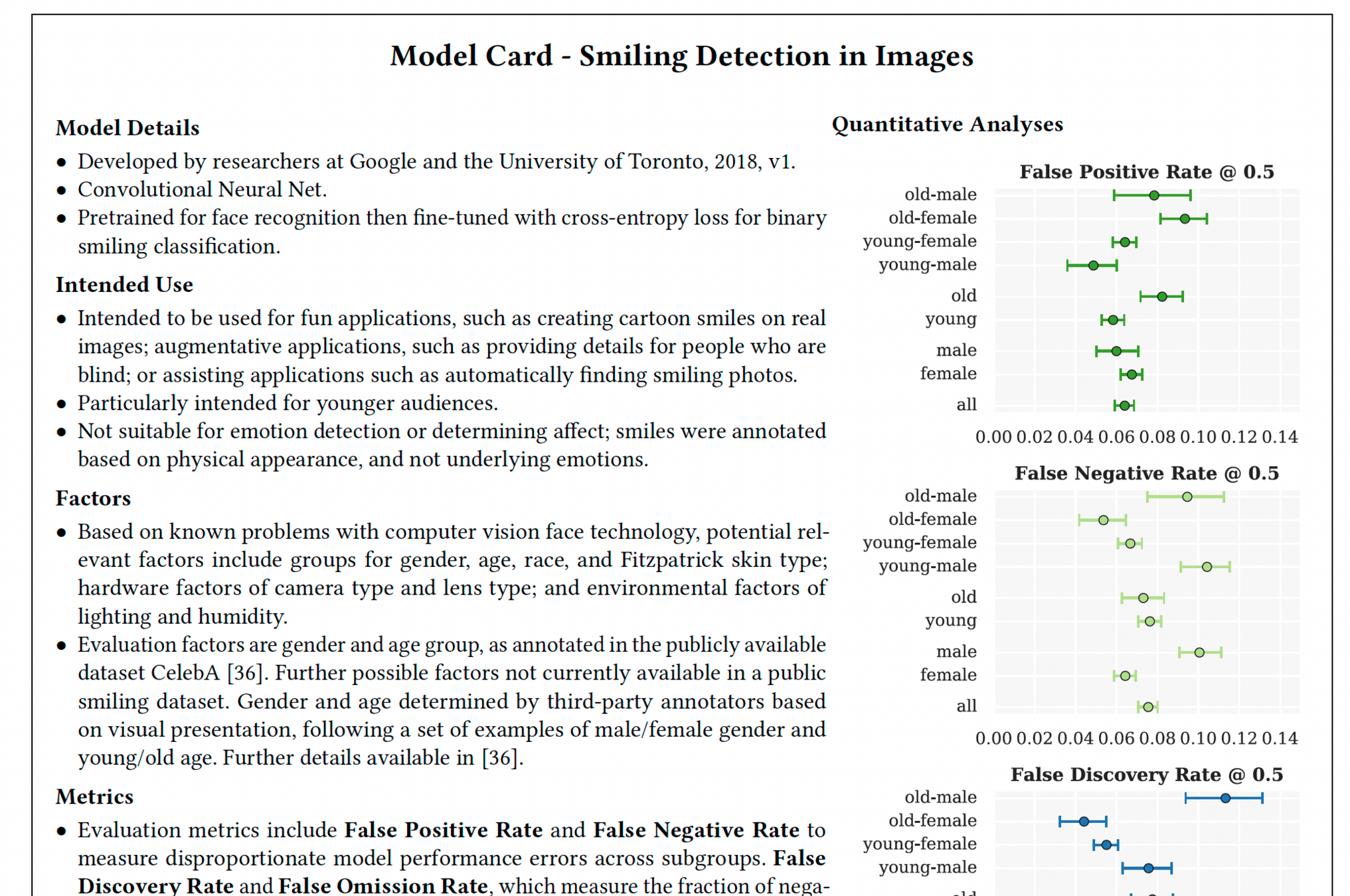
Model Details. Basic information about the model.
– Person or organization developing model
– Model date
– Model version
– Model type
– Information about training algorithms, parameters,
fairness constraints or other applied approaches,
and features
– Paper or other resource for more information
– Citation details
– License
– Where to send questions or comments about the model
Intended Use. Use cases that were envisioned during development.
– Primary intended uses
– Primary intended users
– Out-of-scope use cases.
Factors.
Factors could include demographic or phenotypic
groups, environmental conditions, technical attributes, or
others listed in Section 4.3.
– Relevant factors
– Evaluation factors
Metrics. Metrics should be chosen to reflect potential realworld
impacts of the model.
– Model performance measures
– Decision thresholds
– Variation approaches
Evaluation Data. Details on the dataset(s) used for the
quantitative analyses in the card.
– Datasets
– Motivation
– Preprocessing
Training Data. May not be possible to provide in practice.
When possible, this section should mirror Evaluation Data.
If such detail is not possible, minimal allowable information
should be provided here, such as details of the distribution
over various factors in the training datasets.
Quantitative Analyses
– Unitary results
– Intersectional results
Ethical Considerations
Caveats and Recommendations
HMIA 2025
PRE-CLASS
Zazen Codes Model Cards for Model Reporting [15m]
According to the video transcript, what is the main reason model cards are considered essential in machine learning?
A. They improve model training speed and reduce
coding errors.
B. They make it easier to convert models into
production-ready APIs.
C. They promote transparency, accountability, and
ethical awareness by documenting how models
work, their intended uses, and limitations.
D. They automatically correct data bias during the
training process.
To read a model card, first understand its purpose is to provide transparency and guidance on an AI model, similar to a nutrition label. Then, review the sections, which typically cover the model's basic details (name, version), intended use and limitations, evaluation metrics and data, training data information, and ethical considerations, including potential biases and fairness evaluations.
1 Introduction
2 Safeguard Results
3 Agentic Safety
4 Alignment Assessment
5 Welfare Assessment
6 Reward Hacking
7 Responsible Scaling
What is CBRN?
Get Your Dialog Working
Walk your neighbor through it
Scan the chapter your section came from and identify 5 concepts/terms that we should know.
What is sandbagging?
What is on Anthropic's alignment fails list?
window.dialogData = [
{
"speaker": "Assistant",
"text": "<p>Section 2.6 of the <em>Claude 4 System Card</em> is titled “Bias evaluations.” If that's the section you meant, why don't you start by telling me what issues you think this section is addressing? Or if I've got the wrong one, let's get that straightened out first.</p>"
},
{
"speaker": "Human",
"text": "<p>It seems they want to measure/detect the degree to which the substance of Claude's responses are biased in certain ways. They talk about political and discriminatory bias. My first thought is whether those are the only two kinds of bias we should be worried about.</p>"
}
]systemCardTalkn_n.js.js
chapter
section

HMIA 2025
PRE-CLASS
Get a Receipt
HMIA 2025
CLASS
HMIA 2025
Resources
"The Checklist" by Atul Gawande The New Yorker December 2, 2007
Book The Checklist Manifesto on Internet Archive
Chapter 2 from The Checklist Manifesto "The Checklist" pp. 32-47.
Chapter 4 from The Checklist Manifesto “The Idea” pp 72-85
Review pages from Perrow on Weber's bureaucracy and Weber himself on recordkeeping(in FILES).
The Shuttle Inquiry (NYT pdf in FILES)
Sections on auditing in Data and Society Algorithmic Accountability 2018
Metaxa et al. 2021 "Auditing Algorithms", Foundations and Trends® in Human-Computer Interaction: Vol. 14, No. 4, pp 272–344. DOI: 10.1561/1100000083. Sections 1.1 What is an audit? 1.2 Differentiating Algorithm Audits from Other Testing 3.1 What is an Algorithm Audit? 3.2 Algorithm Auditing Domains
Ryan Notification Norms